


How Can I Minimize Scars in My Child?
By Dr. Eddie Kubek, Carolinas Cleft & Craniofacial Institute
 Plastic surgeons spend years of training to learn how to minimize, camouflage, avoid or revise scars. This article passes on some of this knowledge, explaining what a scar is, answering common questions and sharing a few plastic surgery insights with parents.
Plastic surgeons spend years of training to learn how to minimize, camouflage, avoid or revise scars. This article passes on some of this knowledge, explaining what a scar is, answering common questions and sharing a few plastic surgery insights with parents.
Skin has three basic layers: the epidermis (the outer, visible layer), the dermis (the middle layer), and the hypodermis (the inner layer). Injuries to the epidermis only, such as a sunburn, will not leave a scar. But any injury involving the dermis, including surgical incisions, will heal with a scar.
The dermis is strong yet flexible. Your body repairs it by weaving a network of new elastic fibers to the healing edges of a wound, then pulls them together. However, the new fibers do not blend seamlessly with the original pattern. This is why a scar remains visible.
Although the new fibers will never completely match the old, there are a variety of ways to minimize scars, and several factors involved in optimal healing:
- Diet – As with all aspects of our lives, healing starts with a healthy diet. This means minimizing processed foods, high fructose corn syrup and artificial additives. It is important to maintain a healthy diet over time, because although healing may appear to take only a few weeks, the entire process lasts 12 months and beyond.
- Contamination – Dirt and grime in a new cut can lead to infection and poor wound healing. If your child suffers a deep cut, rinse it with a little soap and a lot of water, and remove any sand and grit. Some bleeding is okay and actually helps the healing process. If there is bleeding, hold pressure (about twice what it takes to make the skin under your fingernail turn white) with a towel for about 20 minutes. With bleeding slowed or stopped, apply a topical antibiotic like Neosporin. You should see a physician as soon as possible, but if you can’t, many cuts can be closed nicely even 24 hours later after the injury.
- Sun exposure – Please know that protecting a healing scar from the sun leads to a better color match when it is healed. Remember to use sunscreen. A minimum of SPF-30 is required, and should be applied even when wearing clothing, since the SPF of most materials is no more than eight to 10.
- Location – For any facial cuts on a child (with the exception of the scalp), it is normal to request a consultation with a plastic surgeon. You can save time, frustration and money by proceeding with item #2 above, then going directly to a children’s hospital or level 1 trauma center. This is because small hospitals and urgent care facilities are rarely staffed by plastic surgeons. When it comes to managing cuts, difficult areas of the body, even for plastic surgeons, include the chin, chest, neck, upper arm, lower eyelid and shoulders.
- Topical therapies – Creams, oils and silicone sheets are the most common topical therapies. Of these, clear silicone sheets worn over the scar for several weeks provide the most effective therapy. Inexpensive products like plain Vaseline® or sesame seed oil can soften scars, as can more expensive products like Mederma®.
- Massage – Probably the most reliable way to improve the appearance and texture of scar fibers is to firmly massage the scar using one of the oils or creams noted above. Beginning at about four weeks for new scars, and anytime for old scars, use your fingertips or thumb to firmly massage the scar vertically, horizontally and in circles several times per day. As with all other therapies, this must be done consistently for several weeks to soften or flatten a scar.
- Laser – Laser therapy is best for scars that remain red beyond 14 months. Please know that the treatments are expensive and are often not covered by insurance. Laser treatments require many repeat visits to the doctor, and unfortunately, results can vary widely.
Despite all efforts, scars sometimes remain quite bothersome. At this point you can consider a consultation with a plastic surgeon for revision. The strategies of surgical revision are to remove the scar and meticulously re-close the skin, re-orient the scar’s direction, camouflage the scar in natural shadows and creases, move it to a less visible location or replace a large area of scar using tissue expansion, or lastly, lengthen the scar (so it no longer pulls on the normal tissue) by changing its geometry.
Dr. Eddie Kubek is a plastic surgeon dedicated to pediatric and adult plastic surgery. He trained at Carolinas Medical Center and the University of Colorado. He is a partner with Dr. David C. Matthews. Their practice in Dilworth has served Charlotte area families for more than 25 years.
This blog was produced in partnership with Charlotte Parent. Click here for the original post and other parenting resources.
Zika, Pregnancy and Birth Defects
By Dr. Amina Ahmed, Levine Children’s Hospital
 Zika virus disease has been front and center in the news this year, but there are still many aspects of the disease – and ways to protect against it – that people may not understand. In some cases, the virus has been associated with Guillain-Barré Syndrome (GBS), a neurological illness that results in temporary muscle weakness or paralysis.
Zika virus disease has been front and center in the news this year, but there are still many aspects of the disease – and ways to protect against it – that people may not understand. In some cases, the virus has been associated with Guillain-Barré Syndrome (GBS), a neurological illness that results in temporary muscle weakness or paralysis.
But of most concern to parents and women of childbearing age is that the virus has been scientifically linked to fetal brain defects that result in congenital microcephaly (which includes such symptoms as an abnormally small head and incomplete brain development). It is still unknown how often the virus is transmitted from the infected pregnant woman to the fetus or how severely the newborn may be affected. Outcomes range from mild delay in development to motor or intellectual deficits or cerebral palsy.
As of May 2016, 195 pregnant women in the United States had laboratory evidence of Zika virus infection. The first case of congenital microcephaly reported in the U.S. occurred in January 2016 in Hawaii in a baby born to a woman who lived in Brazil during pregnancy.
People who have traveled to or lived in areas with transmission of Zika virus are often anxious to be tested. Disease is suspected based on the individual’s symptoms, and a recent history of residence or travel to an area with active transmission of the virus.
For those with these risk factors, infection can be confirmed by laboratory testing of blood or other bodily fluids such as urine. There are two types of tests available: polymerase chain reaction (PCR), which detects the virus, and serology, which detects antibodies (the body’s immune response to the virus). Using guidelines from the Centers for Disease Control and Prevention (CDC) based on the type of exposure and the duration of symptoms, a doctor can determine which test(s) to use for diagnosis. For pregnant women who have traveled to areas with ongoing Zika virus transmission, the CDC recommends testing during the first week of illness. The CDC also recommends testing pregnant women even without symptoms between two to 12 weeks after exposure.
Fortunately, Zika virus infection is usually mild and requires no specific treatment. People with the infection should get plenty of rest, drink fluids and use common medicines such as acetaminophen for fever and pain.
Precaution is key. Those planning travel to areas with Zika virus outbreaks, especially pregnant women and women planning to become pregnant, should check with their doctor regarding the safety of travel. Travel notices are available on the CDC website. It is recommended that women who travel to a country with Zika transmission should not plan to become pregnant for at least eight weeks after leaving. Men who travel to a country with Zika transmission should use condoms or avoid having sex with a pregnant partner. Men should also not have unprotected sex for at least eight weeks after leaving the country, or a full six months if they have symptoms or confirmed infection.
Even if you are not looking to become pregnant, it is important to remember that Zika can still make you very sick. Without an antiviral treatment or vaccine to treat Zika virus, the most critical preventative measure is to protect yourself against mosquito bites when traveling to or residing in areas of active transmission.
Remember:
- Protection is required all day. Wear light-colored clothing that covers as much of the body as possible.
- Use window screens, close doors and windows, and use air conditioning when available.
- Sleep under mosquito nets.
- Use insect repellents containing DEET, IR3535 or icaridin/picaridin.
- Additional information regarding protection against Zika is available on the CDC website.
Dr. Amina Ahmed is a pediatric infectious disease specialist at Levine Children’s Hospital. Her areas of expertise include congenital infections and tuberculosis. Dr. Ahmed is involved in clinical care, teaching and research.
This blog was produced in partnership with Charlotte Parent. Click here for the original post and other parenting resources.
Zika Virus: What is it?
By Dr. Amina Ahmed, Levine Children’s Hospital
 By now, most people have heard about Zika virus disease, which last February was declared a “public health emergency of international concern.” Transmitted by mosquitoes, Zika virus was first identified as a cause of human disease in 1954, which later spread through Africa, Southeast Asia and the Pacific Islands. Only recently has it been identified as a cause of major outbreaks.
By now, most people have heard about Zika virus disease, which last February was declared a “public health emergency of international concern.” Transmitted by mosquitoes, Zika virus was first identified as a cause of human disease in 1954, which later spread through Africa, Southeast Asia and the Pacific Islands. Only recently has it been identified as a cause of major outbreaks.
The current outbreak began in Brazil in early 2015; by the end of the year, it had spread to 33 countries in the Americas and the Caribbean. Among U.S. territories, Zika virus disease has been reported in Puerto Rico, the U.S. Virgin Islands and American Samoa. No locally acquired cases have been reported in the continental United States; all of the approximately 700 cases reported in the U.S. as of June 8, 2016, occurred in those who traveled to areas with active transmission. It is difficult to know how and where Zika virus will spread over time, so it is important for parents to know how to protect themselves and their children from the disease.
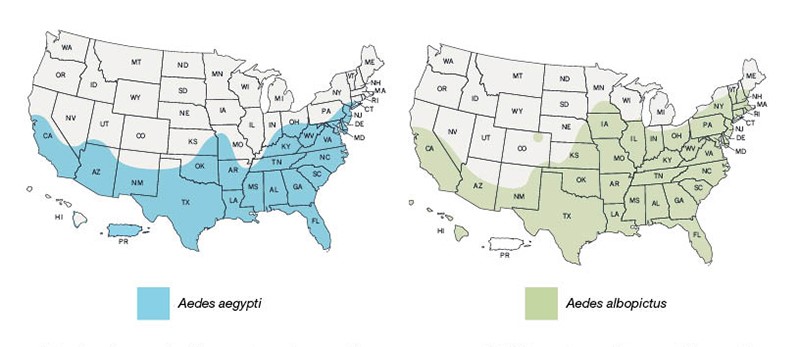
The virus is spread mainly by the bite of Aedes mosquitos, which are found throughout the Americas, including parts of the United States. Mosquitoes become infected when they feed on a person already infected by the virus, and then spread the virus to other people through bites. The virus can also be passed from a pregnant woman infected with the virus to her fetus during pregnancy or around the time of birth. We now know that the virus can be spread by sexual transmission from a man to his partners, and that the transmission can occur before, during or after the man has developed symptoms of the disease. It is also possible for the virus to be spread through blood transfusion, although no such cases have been reported to date. No matter how a person is infected, they can spread the virus by mosquito transmission for a week after being infected; in semen, the virus may persist for at least two weeks.
Fortunately, only one in five people infected with Zika virus actually develops symptoms; the remainder may not even know they have the infection. Characteristic symptoms in adults and children include fever, rash, muscle and joint pain, headache and conjunctivitis (red eyes). The illness is usually mild and lasts two to seven days. People are typically not ill enough to require hospitalization, and death is rare.
Please note that because there is no antiviral treatment or vaccine for the Zika virus, protection against mosquito bites is a key measure to prevent infection for those traveling to or residing in areas of active transmission. Aedes mosquitoes bite mostly during the daylight hours, so protection is essential all day. Such protection includes wearing clothes (preferably light-colored) that cover as much of the body as possible, using physical barriers such as window screens, keeping doors and windows closed, using air conditioning when available, sleeping under mosquito nets, and using insect repellants containing DEET, IR3535 or icaridin/picaridin.
For women who are pregnant or may become pregnant, precautions are different. Read more in Part 2: Zika, Pregnancy and Birth Defects.
Dr. Amina Ahmed is a pediatric infectious disease specialist at Levine Children’s Hospital. Her areas of expertise include congenital infections and tuberculosis. Dr. Ahmed is involved in clinical care, teaching and research.
This blog was produced in partnership with Charlotte Parent. Click here for the original post and other parenting resources.
 As a parent, it’s very hard not to be concerned when your child isn’t feeling well or tells you that they feel something “weird” in their body. When your tween or teenage girl comes to you saying that she feels a lump in her breast, your mind may immediately race to breast cancer. Please know that it is extremely rare for breast cancer to occur in girls younger than 20 years old, accounting for less than one-tenth of one percent of all breast cancers, according to the American Pediatric Surgical Association.
As a parent, it’s very hard not to be concerned when your child isn’t feeling well or tells you that they feel something “weird” in their body. When your tween or teenage girl comes to you saying that she feels a lump in her breast, your mind may immediately race to breast cancer. Please know that it is extremely rare for breast cancer to occur in girls younger than 20 years old, accounting for less than one-tenth of one percent of all breast cancers, according to the American Pediatric Surgical Association.
With today’s heightened awareness around breast cancer, more and more doctors are seeing girls concerned about lumps they feel in their breasts. These lumps are actually normal breast tissue that is growing at different rates. Since younger breast tissue is denser than more mature tissue, it can be fibrous and have a nodular feel. A mass in the breast of a young girl is very different than a mass in an adult, and is best evaluated by a pediatric surgeon to avoid unnecessary tests and procedures. Due to this density of teenage breast tissue and the rarity of breast cancer in this age group, mammography should not be used, because it exposes the patient to radiation and is not a reliable screening tool for breast cancer in young women. Sometimes an ultrasound may be recommended, but an experienced pediatric surgeon should be able to evaluate the situation just as carefully.
If your child does feel a lump, you may be told that it is a benign fibroadenoma, the most common diagnosis for breast lumps in adolescent females, and which is likely the result of abundant estrogen. These are firm, rubbery lumps within the breast tissue that are not attached to skin or muscle and may move when touched. The size of the lumps may fluctuate in size with monthly menstrual cycles. Treatment can vary. It may be as simple as monitoring the lumps for size and texture, and in the most extreme cases, a biopsy or surgery may be necessary. Fortunately, there is little risk of fibroadenomas progressing to breast cancer over time, and fibroadenomas alone do not increase the risk of breast cancer.
So if your daughter is concerned about something she feels in her breast, take comfort in the fact that lumps in teenage breast tissue are usually benign. A pediatric surgeon can provide complete reassurance, and will help determine if any additional testing or procedures are needed. Remember to applaud your daughter for being aware of changes in her body, and encourage her to always come to you to discuss her feelings and concerns about every stage of her development.
This blog was produced in partnership with Charlotte Parent. Click here for the original post and other parenting resources.
Chest Wall Deformity: More Common Than You Think
 Now that the weather is getting warmer, pediatric surgeons are seeing an increase in referrals to correct a surprisingly common but little-discussed condition: chest wall deformity.
Now that the weather is getting warmer, pediatric surgeons are seeing an increase in referrals to correct a surprisingly common but little-discussed condition: chest wall deformity.
The appearance of chest wall deformities can vary: the condition is either “sunken in” (officially known as Pectus Excavatum) or “sticking out” (Pectus Carinatum). Unless the case is severe, you may not even notice it until you see your child shirtless. Often, such deformities are milder in the early years and do not become pronounced until children hit growth spurts in their late adolescent and teen years. Personally, I dislike referring to these conditions as “deformities” at all. The negative connotations are not warranted. These conditions are frequent enough to occur in one out of every 1000 children, and commonly require no treatment.
Pectus Excavatum affects the sternum (breastbone) and the cartilage that connects the sternum to the ribs. The abnormal growth of the cartilage results in an indentation in the middle of the chest. The condition has a wide range of severity, from a very mild depression to a severely sunken chest. Depending upon the severity, patients with Pectus Excavatum may have no physical symptoms or may have shortness of breath during exercise, as well as chest pain and/or palpitations. This is due to compression of the heart and lungs by the more severe indentations. We encourage all families to consult with a pediatric surgeon. Surgical repair is a major decision and education is essential. Insurance carriers frequently require additional studies before approving surgery. During surgery, a metal bar is inserted into the chest to raise the breastbone and allow the cartilage to regrow and solidify into a more normal shape (usually in one to three years). The bar is then removed with an additional minor procedure.
Pectus Carinatum is the result of the sternum and cartilage protruding. Frequently referred to as “bird chest,” Pectus Carinatum is less common than Pectus Excavatum. When Pectus Carinatum becomes more pronounced after a growth spurt, it may be painful, and the protrusion may be noticeable through a child’s clothing. At Pediatric Surgical Associates, we often recommend non-operative treatment options and help make the appropriate referrals.
It is important to emphasize that these conditions are not life-threatening, but for children who deal with either, the psychological toll on their body image and confidence can be profound. We often see children, especially boys, who become very self-conscious about their condition. They may avoid sports or activities where they might need to undress in a communal space, and tend to stay away from beach trips and pool parties. Girls going through puberty may struggle with what appears to asymmetrical breast development, when the problem is really with the underlying chest wall.
For those children whose condition is relatively mild and does not limit them physically, surgery is not necessary. I am often impressed with children who choose to “own” their condition. If others stare or ask questions, these children use this as an educational opportunity to explain chest wall deformity and how common it is.
For those families considering surgery, summer is the time to do it. The hospital stay for surgery (especially for Pectus Excavatum) is typically four to five days, and physical activity is highly restricted for an extended period of time.
If you are concerned that your child may have a chest wall deformity or you are seeking treatment, please visit our website for more information or to schedule a consultation.
This blog was produced in partnership with Charlotte Parent. Click here for the original post and other parenting resources.
Abdominal Pain: When To Call The Doctor
 “My tummy hurts!” When most parents hear these words, they brace for a rough few days of a stomach bug (gastroenteritis), or vomiting and diarrhea caused by something their child ate. In some cases, belly pain can be explained by simple constipation. In other cases, it can be something worse – appendicitis.
“My tummy hurts!” When most parents hear these words, they brace for a rough few days of a stomach bug (gastroenteritis), or vomiting and diarrhea caused by something their child ate. In some cases, belly pain can be explained by simple constipation. In other cases, it can be something worse – appendicitis.
The first symptoms of appendicitis generally include pain around the belly button. Other symptoms can include vomiting, nausea and loss of appetite. Unlike the less serious causes of abdominal pain mentioned above, appendicitis pain usually worsens and, within the first 12-24 hours, moves to the lower right side of the belly. If this happens, it’s important to consult a doctor as soon as possible.
So what is the appendix? It’s a small finger-shaped intestinal organ that sits at the beginning of the large intestine, just past the transition from the small intestine to the large. No one is really sure why we have this appendage. There is evidence to suggest that early humans needed it to aid in digestion, but today the appendix is completely unnecessary.
Appendicitis occurs when this organ becomes infected. Approximately 80,000 children in the United States suffer from appendicitis every year, and most of them are between the ages of six and 18. The standard treatment for typical appendicitis is a short and simple operation to remove the appendix before the appendix ruptures, which usually happens after symptoms have lasted 48-72 hours.
Appendicitis is the most common reason for emergency surgery in children. Although the thought of an operation is scary, it needn’t be thanks to laparoscopy, or minimally invasive surgery. With very small and specialized tools and scopes, pediatric surgeons can remove an infected appendix with a few small incisions. The average procedure time is 30 minutes, and most children with typical appendicitis go home the next day. Studies have been performed to determine if some children with appendicitis can be safely treated with antibiotics and not surgery. The complication rates in children treated without surgery are unacceptably high, and laparoscopic appendectomy remains the preferred treatment for children with typical appendicitis.
In about 20 percent of cases, the appendix will be perforated at the time of diagnosis, which means there is a small hole in the wall of the appendix. This is also known as a “ruptured” or “burst” appendix. When it occurs, the infection from inside the appendix leaks out into the abdomen. Children experiencing this condition usually have a longer recovery and are best treated with an extended course of antibiotics. Many children with perforated appendicitis receive surgery at time of diagnosis, but sometimes, if the appendix has been perforated for an extended period of time, the best treatment is initially just antibiotics, followed by “interval appendectomy” after the infection resolves. Interval appendectomy is usually out-patient surgery performed eight to 12 weeks after the initial diagnosis.
For many parents, appendicitis is their first exposure to pediatric surgery. They may not know what to ask when a surgeon is referred to them. Please remember that it is your right to choose the surgeon who will operate on your child, and you should feel very confident in your pediatric surgeon’s abilities. To ensure the best outcome, look for a board-certified pediatric surgeon. Then ask as many questions as you need to feel comfortable.
This blog was produced in partnership with Charlotte Parent. Click here for the original post and other parenting resources.
By Dr. Joe Molitierno, Pediatric Urology Associates
 Bedwetting is a common problem that can cause a great deal of stress and anxiety. Parents are often concerned that there is something wrong with their child because they have accidents at night. Children are often embarrassed by their bedwetting and hesitant to go to sleepovers and sometimes even worried about taking naps.
Bedwetting is a common problem that can cause a great deal of stress and anxiety. Parents are often concerned that there is something wrong with their child because they have accidents at night. Children are often embarrassed by their bedwetting and hesitant to go to sleepovers and sometimes even worried about taking naps.
It is important to note that bedwetting is a very normal part of development for many children. Nearly 25 percent of five year-old children wet the bed, and this decreases to less than five percent by the age of 10. Most experts agree that there is about a 15 percent chance of outgrowing bedwetting each year. Bedwetting can sometimes be genetic, and children of bedwetters have a greater than 40 percent chance of being bedwetters themselves.
The underlying causes can vary. Most often the communication between the brain and the growing bladder just needs more time to mature. In rare cases, there is a serious underlying disease process such as neurologic cause or diabetes, which can lead to new occurrences of bedwetting in a previously dry child. But in most cases, nighttime wetting is due to urine holding for long periods during the day, dietary triggers, and drinking a great deal of fluid late in the day. Another factor is underlying constipation that compresses the bladder, making it hold less volume and causing irritation. Children with overactive bladders and resulting daytime urinary frequency will often wet the bed until they either outgrow their overactive bladders or treat their symptoms with medication. Even in these cases, the nighttime wetting usually lags behind the resolution of daytime symptoms.
The evaluation for bedwetting should never begin before five years of age, and most physicians don’t routinely evaluate children before the age of seven unless they have both day and nighttime symptoms that are impairing daily activities or they are experiencing new onset. Evaluation includes a thorough physical examination, discussion of diet and voiding habits during the day, and a thorough evaluation for constipation. A urinalysis may be useful but is not always necessary. Imaging is not usually performed in the evaluation of isolated nighttime wetting unless there are also daytime symptoms or the patient has failed multiple therapies.
The treatment for nighttime wetting begins with a combination of bowel and bladder retraining and dietary modifications. We encourage urination every two hours during the day, and often we have the child “count to ten and pee again” to ensure he or she is completely emptying the bladder. Dietary modifications include the removal of caffeine, carbonation and artificial red dyes from the diet. Drinking after dinner should be limited to only sips of water if needed, and consuming milk products and foods and drinks with a high sodium content should be restricted late in the day because this leads to an increased urine production at night.
Please note that punishment has NO role in the treatment of bedwetting. Positive reinforcement is important because children usually feel embarrassed about their situation and this affects their self-esteem. Additionally, leaving a child in a Pull-Up overnight does not encourage nighttime wetting or extend its duration, and in fact may help make the child feel better and more comfortable than needing their sheets and clothes laundered frequently.
If these conservative measures are unsuccessful, a pediatric urologic evaluation is often necessary. Alarm systems or medications may be useful in helping some children stay dry, while other children may need a combination of therapies. But in every case, the mainstay of treatment is bowel and bladder retraining, treatment of constipation and dietary modifications.
If you have any questions or concerns about bedwetting, never hesitate to discuss with your pediatrician.
Joe Molitierno, MD is a board-certified Pediatric Urologist who trained at both UNC Chapel Hill and Emory Schools of Medicine. He has been practicing in the Charlotte area for over nine years. He is a partner with Pediatric Urology Associates, PA and is the director of the Nocturnal Enuresis and Wetting Treatment (NEWT) center, the Carolinas first pediatric voiding dysfunction center.
This blog was produced in partnership with Charlotte Parent. Click here for the original post and other parenting resources.
Stretching and Activity for Children
By Dr. Virginia F. Casey, OrthoCarolina Pediatrics
 We all know that activity and exercise are essential components of a healthy lifestyle. They are particularly important for our children, because early exposure to exercise can lead to a positive habit into adulthood. As physicians, we encourage children to actively move their bodies at least one hour every day. This can take many forms: running around outside, playing tag, riding bikes or playing on a playground. Healthy activity can also come from more formal activities such as team sports, dance or karate. Participating in physical activities not only helps children grow into strong and fit adults, it also helps them concentrate better in school and succeed in almost all areas of life in those critical early years.
We all know that activity and exercise are essential components of a healthy lifestyle. They are particularly important for our children, because early exposure to exercise can lead to a positive habit into adulthood. As physicians, we encourage children to actively move their bodies at least one hour every day. This can take many forms: running around outside, playing tag, riding bikes or playing on a playground. Healthy activity can also come from more formal activities such as team sports, dance or karate. Participating in physical activities not only helps children grow into strong and fit adults, it also helps them concentrate better in school and succeed in almost all areas of life in those critical early years.
As parents, how do we know which physical activities are best for our children? The good news is almost any activity that keeps kids moving is beneficial, but there are a few tips you should keep in mind:
- Variety is extremely important.
- Formal stretching helps to avoid injury.
- At least one activity that focuses on core strength (tummy and back) is necessary.
Let’s start with why variety is so critical. Participating in different activities helps ensure more symmetric development of muscles and decreases overuse injuries by giving some muscle groups a rest while working others. For example, I see a lot of soccer players with hip flexor strains. Sometimes this occurs because the kids’ only activity is playing soccer. They play 10 hours a week and do not give their hip flexor (one of the big kicking muscles) time to rest or stay balanced with other muscle groups. I definitely do not want to pick on soccer, because my children love it, but this is an example of the narrow range of activity that applies to many sports. If we balance soccer with swimming as one possible combination, then the hips are still working hard and getting stronger, but are not using the same muscle groups over and over again. Variety helps prevent overuse injuries.
Such injuries also stem from a lack of stretching. Parents and coaches often assume that youth and flexibility provide protection from injury. That is simply not the case. Kids are actually at more risk for overuse injury due to their growing skeletons. The tendons and ligaments tend to be stronger than the growth plates, where overuse syndromes can occur. We commonly see this in the heel (Severs) and knee (Osgood-Schlatters). Fortunately, routine stretching can help prevent these problems.
I recommend that kids stretch before each organized activity, to get the blood flowing and the muscles warm. Warm-up activities should increase the heart rate without stretching the muscles too much. Jumping rope does this nicely, as does a simple jog – but not a sprint which stretches the muscles too much before they are warm. Once the muscles are warm, the kids should go through a stretching routine that hits the major muscle groups in the arms, legs and core. Only then are the kids ready to play. This may seem like a waste of time to an impatient coach who has a lot of skills to teach, but it is very important to keep the players healthy and playing at their best. Practice should conclude with a stretching routine as well. This type of injury prevention routine will help keep kids on the playing fields and out of the doctor’s office.
Finally, I want to stress the importance of core strength. Most of us already recognize that having a strong core helps prevent back injuries and improves overall function. As one example, knee pain due to patellar tracking problems can improve by building core strength. Balance and agility are related as well. There are many beneficial activities that focus on the core, including yoga, Pilates, martial arts and gymnastics.
The take-home message is to encourage your child to participate in physical activities or sports for an hour a day. Incorporate more than one sport or activity, including one that develops core strength, and encourage stretching on a regular basis. Effective exercise routines contribute to a healthier childhood with fewer overuse injuries.
Dr. Virginia F. Casey, MD, OrthoCarolina Pediatrics, is versed in all areas of pediatric orthopedic conditions, from simple strains to complex reconstructive hip surgery. Her practice includes newborns, adolescents and young adults. She has a special clinical interest in hip disorders.
This blog was produced in partnership with Charlotte Parent. Click here for the original post and other parenting resources.
How Afraid Should We Be of MRSA?
 By now you’ve probably heard about or known someone who has contracted MRSA. These experiences can range from fairly common skin infections to horrible stories of children who suffer lasting harm from serious MRSA-related illnesses. As a physician, I hear this question from concerned parents all the time: “How scared should I be?”
By now you’ve probably heard about or known someone who has contracted MRSA. These experiences can range from fairly common skin infections to horrible stories of children who suffer lasting harm from serious MRSA-related illnesses. As a physician, I hear this question from concerned parents all the time: “How scared should I be?”
Most parents will be glad to know that serious MRSA infections are rare, and most can be treated easily. But serious cases do happen, and the number could continue to grow as the medical community struggles with what to do about antibiotic resistance. The good news is that you can play an active role in minimizing your risk.
MRSA is an acronym for methicillin-resistant Staphylococcus aureus, which is a type of staph bacteria. Multiple strains of staph bacteria are quite common in the environment, and all of us have staph bacteria living harmlessly on our skin or in our noses. Staph bacteria can enter the body through the skin via cuts, scrapes or rashes, and can cause minor skin infections. Most are self-limited and heal on their own if the wound is kept clean, but sometimes antibiotics are needed if signs of infection develop.
The MRSA strain is different from other staph bacteria because of its resistance to most of the antibiotics that have traditionally been used to treat staph infections. Methicillin is one of many antibiotics to which MRSA has developed resistance and is no longer effective in treating infections. When bacteria become resistant to antibiotics, they are harder to kill and it becomes more difficult to treat infections. Bacteria become resistant by changing in ways that affect the ability of the antibiotics to work effectively.
How do you keep your child safe and help doctors curtail antibiotic resistance?
- Be patient. If your child is sick, give them an opportunity to fight colds and upper-respiratory viruses. Antibiotics will only help if bacteria are causing a sinus or ear infection (typically after several days of illness).
- Follow instructions. Take antibiotics as the doctor has prescribed them. If you are supposed to take a 10-day course or finish all of the medication, then do so. Do not hoard antibiotics for future use.
- Leave it to the professionals. Do not “put yourself on antibiotics” if you have some left over from a previous illness.
- Wash your hands with ordinary soap and don’t use antibacterial soap that contains the ingredient triclosan. The repeated use of triclosan gives bacteria regular exposure to the germ-killing agent to which they can become incrementally resistant.
If your child is genuinely ill and seems to be worsening quickly, do not hesitate to take him or her to the emergency room or urgent care. A serious MRSA infection requires immediate treatment. If you have any questions, never hesitate to call your doctor. You can read more at http://www.kidshealth.org/.
This blog was produced in partnership with Charlotte Parent. Click here for the original post and other parenting resources.
Surviving the Respiratory Virus Season
By Dr. Hugh Black, Asthma & Allergy Specialists
 Each of these viruses has the common feature of causing airway injury, but each can have its own unique set of symptoms:
Each of these viruses has the common feature of causing airway injury, but each can have its own unique set of symptoms:
- Rhinovirus causes sore throat and nasal congestion for most, but can trigger significant wheezing in patients with asthma.
- RSV virus causes head congestion, sore throat and laryngitis in older children and adults. The symptoms can be much more severe in infants, causing significant lower airway infections with difficulty breathing. This condition, called bronchiolitis, is one of the major causes of hospitalization for infants and young children.
- Para influenza causes croup, which is a swelling just below the vocal cords, producing a deep barky cough and difficulty breathing.
- Human meta-pneumovirus causes major airway injury with a wet cough that can last for weeks.
- Influenza has a variety of symptoms including coughing, muscle aches, chills, fever, headache and stomach upset.
Preventing respiratory tract infections in children is difficult. These viruses are spread by contact. Simply touching a contaminated surface and then putting a hand to mouth or nose is enough to cause an infection. Good hand washing is the proven way to decrease the spread of a virus in a household. Medications to prevent these viral illnesses are limited. There is a preventative injectable medication for RSV, but it is only approved for select premature infants or infants with heart disease who are at high risk. Only influenza has a widely available vaccine, which is usually given in the fall and begins providing immunity in most patients a month or so after inoculation. There are oral medications that can be used to treat influenza, but they work best if they are started in the first 48 hours of symptoms. These same medications can be used preventively, to reduce your child’s chances of becoming infected with influenza if you know they have been exposed.
Parents should contact their physician to discuss starting these medications if they or their child have flu symptoms or have been closely exposed to someone with the flu. For most viral illnesses, the cough can be extreme, but cough and cold formulas rarely make a significant difference in the amount of coughing or the speed of the healing process. If a child develops wheezing or labored breathing, or demonstrates a reduced interest in food and water, their primary care provider can guide parents as to the best course of action.
One of the most difficult aspects of respiratory virus season is the frequency with which children can become infected. It is common for children under the age of three to be infected with one of these viruses every three to four weeks during virus season, frequently contracting a new virus before healing from the last. Though viruses are present year-round, summer respiratory infections are less common, giving families a reprieve from June through September before starting the cycle all over again.
Hugh Black, MD, is a board-certified Pediatric Pulmonologist who has been practicing Pediatric Pulmonary and Allergy Medicine in Charlotte for almost 20 years. He practices with Asthma and Allergy Specialists, PA, and is the co-director of both Sleepwell Kids Pediatric Sleep Center and the Western Carolinas Affiliate Cystic Fibrosis Center.
This blog was produced in partnership with Charlotte Parent. Click here for the original post and other parenting resources.
What We Do






Achievements / Associations

